About the review
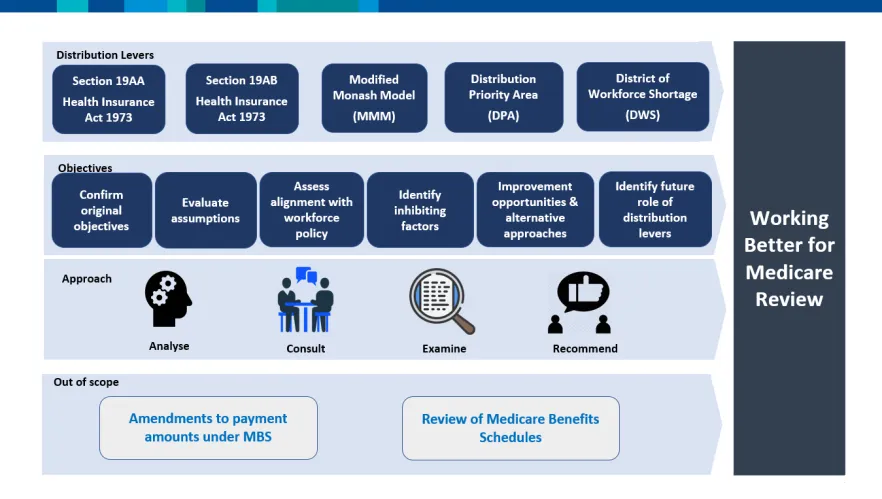
The Working Better for Medicare Review examined the effectiveness of our current distribution levers. These are laws and policies used to encourage or require health professionals to work in areas of workforce shortage. These levers include:
- sections 19AA and 19AB of the Health Insurance Act 1973 (the Act)
- workforce classifications – specifically the Distribution Priority Area (DPA), District of Workforce Shortage (DWS) and the Monash Modified Model (MMM) classifications.
The review is part of our 2023–24 Strengthening Medicare Budget measures (Supporting health, care and support services in thin markets).
Review objectives
The review sought to:
- confirm the original objectives of the distribution levers
- evaluate how appropriate and robust the assumptions underpinning the levers are
- consider and report the value of retaining the levers
- assess how the levers align with current health workforce policies and priorities
- identify key factors and barriers impacting appropriateness and effectiveness
- if appropriate, identify opportunities to improve the way the levers achieve current medical workforce policy aims
- consider, and where appropriate make recommendations on alternative approaches for us to achieve these aims
- identify the future role of the levers.
Distribution levers
Section 19AA
This section of the Act was introduced in 1996. It requires all doctors who are Australian permanent residents or citizens to hold fellowship of a specialist college before they can access Medicare rebates for their patients. In 1996 there were approximately 1,300 medical graduates per year; now there are around 4,000.
Learn more about section 19AA requirements.
Section 19AB
This was introduced as part of the same amendment that established section 19AA. To access Medicare benefits when working in Australia, overseas trained doctors must work for at least 10 years in a DPA (for general practitioners), or a DWS (for non-GP specialists).
The aim was to direct these doctors to public hospitals or areas where there was a shortage of medical workforce. In 1996, there were approximately 600 overseas trained doctors entering Australia each year; now there are around 2,000.
Learn more about section 19AB requirements.
District of Workforce Shortage measure
This measure was established in 2000–01 to support the operation of section 19AB. It is the subject of ongoing friction with the private health sector, with the grounds for exemption expanding over the past 26 years.
Monash Modified Model
The government introduced the MMM in 2015 based on work by Dr John Humphries to develop a more effective framework for providing support and incentives to general practices. The MMM is now used broadly across a range of health, aged care and disability programs as a measure of remoteness.
Distribution Priority Area classification
The DPA classification was established in 2018–19 in response to criticism by general practitioners that the DWS did not effectively reflect patient flows and access to general practice services. Some parts of the sector are concerned about a series of automatic rules being applied.
Lead reviewers
The review was undertaken by independent lead reviewers:
They were supported in this work by expert consultants:
Consultation
The lead reviewers and consultants engaged extensively with internal and external stakeholders through various channels, including consultations, workshops, and written surveys.
Stakeholders consulted include:
- state and territory health departments
- Department of Health and Aged Care
- Services Australia
- Department of Finance
- Department of Home Affairs
- Chief Executives Forum
- Primary Health Networks (PHNs)
- Rural Workforce Agencies (RWAs)
- Australian Medical Association (AMA)
- GP and non-GP specialist medical colleges
- Rural Doctors Association of Australia (RDAA)
- Australian Health Practitioners Regulation Agency (AHPRA)
- Aboriginal and Torres Strait Islander health organisations
- Regional Training Hubs.
We published an online survey on our website to capture feedback about the distribution levers from:
- the general public
- organisations
- health professionals
- government departments.
We received about 300 submissions.
We also conducted extensive internal consultation to provide insight into:
- the operation and administration of the distribution levers
- how they may be impacted by reforms
- potential areas for improvement.
Outcomes
Final report
The final report contains a total of 26 recommendations, and proposes retaining the current levers with:
- significant reform to maximise their effect and efficiency and improve access to health care for all Australians, regardless of where they live
- improved classification systems to better identify areas of workforce shortage
- careful and coordinated implementation of future reform
- the development of robust governance and review arrangements, particularly relating to the processing of exemptions to current requirements
- longer-term strategies to improve training pathways and reliance on international workforce.
In response to 4 recent primary care and workforce reviews, we formed the Primary Care and Workforce Reviews Taskforce. The taskforce will bring together advice to government on an integrated primary care and health workforce reform agenda, considering the findings and recommendations of these reviews.
Resources
Working Better for Medicare Review – Final report and appendices
Terms of reference – Working Better for Medicare Review
Read past editions of the Working Better for Medicare review newsletter.
Contact
