This statement has been archived.
The Australian Health Protection Principal Committee (AHPPC), on the advice of the Communicable Diseases Network Australia, today considered a number of additional public health measures to provide advice to the National Cabinet in relation to strengthening the control of COVID-19 in Australia.
The COVID-19 pandemic has continued to spread globally. Our actions to date, including border measures and extensive case finding and contact management, based on best evidence strategies to contain transmission, have provided time for our health system and society to prepare. These strategies will remain essential throughout the control phase that we are entering, but now need to be augmented by additional social distancing measures that will reduce the spread of all respiratory infections.
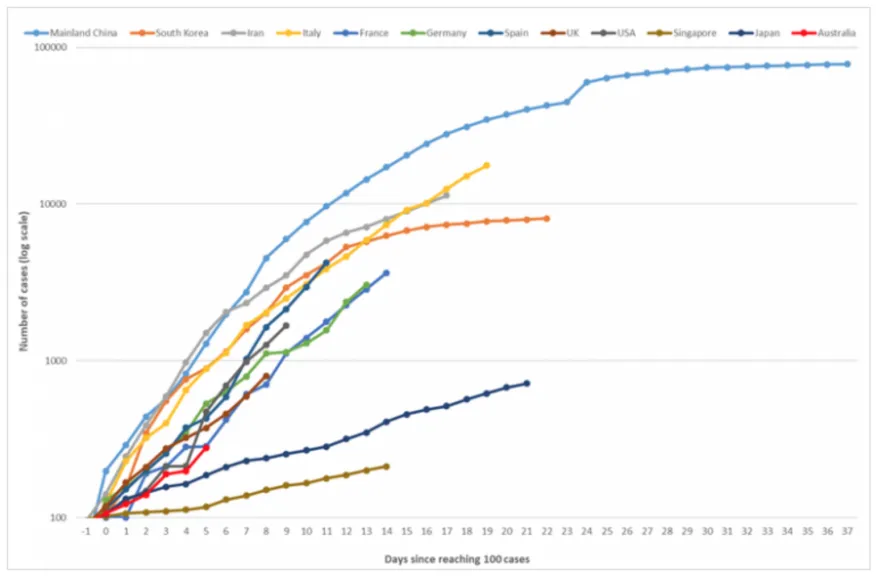
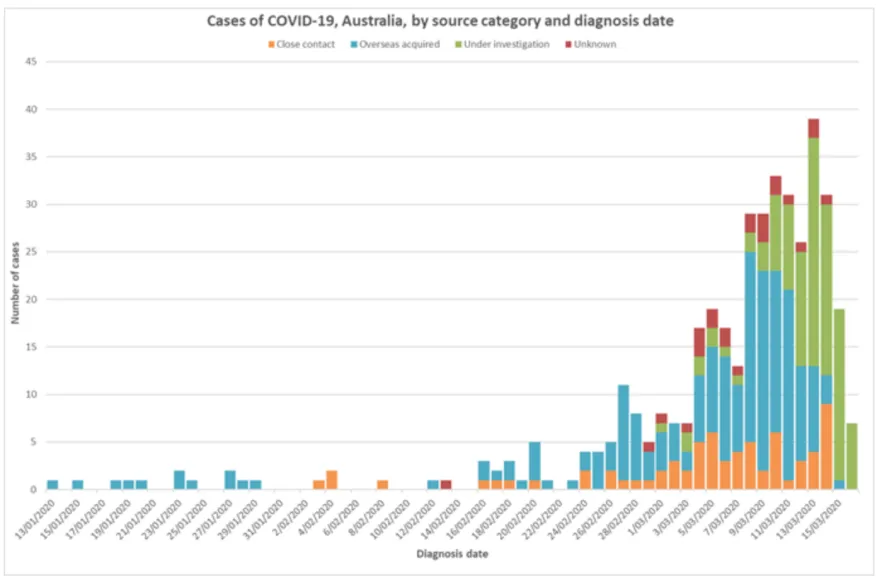
In the absence of a vaccine to provide immunity to the population, these measures are essential to protect the Australian public. Figure 1 shows the current trajectory of the outbreak in Australia compared to other nations experiencing significant COVID-19 outbreaks, with a growing number of cases daily, fuelled by an increase in overseas-acquired cases in the past 30 days (see Figure 2). These case figures have been detected from over 80,000 tests conducted to date, which is high compared to our overseas counterparts. Given the significant increase of cases and experiences of Europe and the United States, the AHPPC feels very strongly that social isolation and distancing measures be enhanced.
COVID-19 is a contagious viral infection that causes mild respiratory illness in most people. Presentation can range from no symptoms to severe illness with potentially life-threatening complications, particularly in people who are vulnerable to infections. The current principle national objective is to slow progression of the outbreak in Australia and limit the burden on our health system by taking measures to reduce transmission.
Transmission of COVID-19 is through contact with respiratory droplets containing the virus, produced when an infectious individual coughs or sneezes. As a consequence, individual behaviour is key to containing spread of the virus, and involves taking personal responsibility for measures, such as regular hygiene practices, early self-isolation and personal social distancing.
Social distancing is one of the key measures currently being utilised to contribute to Australia’s ability to severely limit transmission of COVID-19. This reduces the burden of disease in the community, and importantly, will ensure healthcare capacity is not overwhelmed at any given time. The health sector must continue to undertake its core functions, as well as maintain the capacity to support those with COVID-19 who require more intensive care.
These interventions may need to continue for more than 6 months, and must be feasible and sustainable. The application of extraordinary measures for a short term (for a period of four weeks) will only defer the increase in cases and will not achieve long term flattening of the curve or, ultimately, save lives.
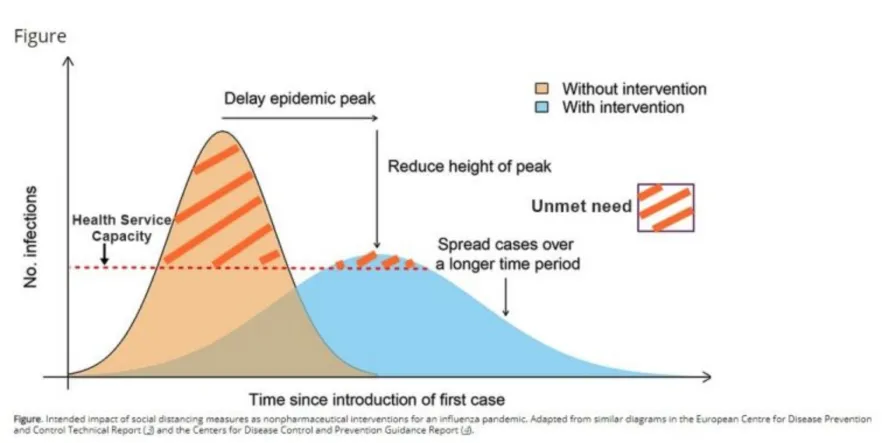
Figure 3 demonstrates the impact of effective social distancing and other interventions on the timing and size of the peak burden of disease. As demonstrated in the figure below, the intent is to ensure the burden of disease does not exceed the capacity of the health system to manage.
The overarching goal of our recommendations is to slow the spread of the virus and flatten the epidemic curve. We all have both a community and individual responsibility to maintain social distancing and minimise interactions in order to protect the people we love. The aim is a population response, to reduce transmission to protect vulnerable populations.
Our approach to containing the COVID-19 pandemic needs to be flexible and scalable to respond effectively to the evolving situation. Whilst we have a national approach to social distancing currently, if case numbers continue to grow, more stringent measures will need to be introduced locally or nationally to control surges in case numbers.
Recommendation to the education sector
Schools
The AHPPC met on Tuesday 17 March to consider the issue of school closures in relation to the community transmission of COVID‑19. The Committee’s advice is that pre-emptive closures are not proportionate or effective as a public health intervention to prevent community transmission of COVID-19 at this time.
There is currently limited information on the contribution of children to transmission of COVID-19. The WHO-China Joint Mission noted the primary role of household transmission and observed that children tended to be infected by adults in the household. In China, 2.4% of total reported cases were under the age of 19 years old. Worldwide, of those cases under 19 years of age, very few were severe or critical. This contrasts distinctly with the severity pattern observed with other respiratory viruses, where young children are particularly at risk of severe disease.
Previous studies suggest that the potential reduction in community transmission from pre‑emptive school closures may be offset by the care arrangements that are in place for children who are not at school. Children may require care from older carers who are more vulnerable to severe disease, or may continue to associate (and transmit infection) outside of school settings.
Broadly, the health evidence on school closures from previous respiratory epidemics shows the costs are often underestimated and the benefits are overestimated. This may be even more so in relation to COVID-19 as, unlike influenza, the impact on otherwise healthy children has been minimal to date.
School closure is associated with considerable costs. Studies have estimated that around 15% of the total workforce and 30% of the healthcare workforce may need to take time off work to care for children. This burden will be significant and will fall disproportionately on those in casual or tenuous work circumstances.
At this stage, the spread of COVID-19 in the community is at quite low levels. It may be many months before the level of Australian community infection is again as low as it is at the moment. For pre-emptive school closures to be effective, closure for at least several months is required and it would be unclear when they could be re-opened.
School closures for shorter defined periods may be considered as part of a suite of more stringent distancing measures later in the outbreak, in anticipation of a peak in infection rates.
Short term reactive school closure may also be warranted to allow cleaning and contact tracing to occur in response to an outbreak in a given school.
More than 70 countries around the world have implemented either nationwide or localised school closures, at different times in the evolution of the local COVID-19 epidemic, however it should be noted the majority of these have not been successful in controlling the outbreak. Some of these countries are now considering their position in relation to re-opening schools.
Singapore has had success in limiting the transmission of COVID-19 in the community without closing schools. Other countries are working in different contexts, including Northern Hemisphere countries making decisions at the end of winter with COVID-19 being accompanied by influenza in the community.
The advice in relation to school closures will continue to be reviewed at daily meetings of the AHPPC.
Schools should implement a range of other strategies to reduce transmission, including the promotion of personal hygiene measures (frequent handwashing, reducing face-to-face contact, cough etiquette), physical distancing, reducing public gatherings (e.g. face-to-face school assemblies), and reducing the mixing of students (e.g. reduced use of common areas, staggered lunchtimes, and reduced after-school activities and inter-school activities).
Schools should also reinforce existing policies to exclude students and staff who are unwell, and current policies requiring quarantine for those who have recently travelled overseas. It is also important that the learning needs of students who are excluded from school are met.
Boarding schools
Boarding schools are at high risk of transmission of COVID-19 due to close and shared living arrangements and higher frequency of face-to-face contact. An outbreak in a boarding school would present a difficult management issue including potentially the isolation of the entire boarding school, as all students and staff would be defined as close contacts following a confirmed case. Depending on the structure, the boarding school may be unsuitable for isolation procedures.
Should a boarding student from a rural or remote community be diagnosed with COVID-19, they may not be able to return home if there is not sufficient health infrastructure to support them, or support their isolation.
Schools and parents should consider the risks versus the benefits of a student remaining in boarding school, and make their own decision, noting that the duration of the COVID-19 pandemic is likely to span more than six months. The decision to remain at boarding school should be a shared and documented decision.
Universities and other higher education centres
University and higher education are considered essential and should continue at this time, but with risk mitigation measures in place. AHPPC considers the actions below will enact social distancing and help to protect health service provision as well as ensuring business continuity:
- Encouraging staff who can work effectively from home to do so.
- Holding as many business meetings as possible by audio-visual link or other remote means.
- Cancelling all non-essential events.
- Encouraging universities and higher education facilities to provide to access online content remotely and participate in as many other classes as possible by audio-visual link or other remote means.
- Ensuring lectures and examinations have no more than one person per four square metres of floor space and have fewer than 100 persons.
- Continuing to support clinical placements if the necessary risk assessments have been undertaken, after discussion with clinical supervisors and facilities. The safety of patients, staff and students is paramount.
- Staff should continue to undertake their normal duties with risk mitigation strategies.
Given the demonstrated feasibility of online delivery of lecture content, we support universities and higher education centres moving to an online platform, where appropriate, for continuity of student education.
For those programs that require face-to-face interactions or utilise the physical environments, such as laboratories, classes can continue but need to consider reduction in the size of the classes; ensure regular hand hygiene for all staff and students (e.g., hand sanitisers at entry points); and ensure cleaning addresses areas of high touch points for students and staff.
These steps will allow universities and higher education centres to play their part in reducing interactions as much as possible in support of the government's efforts to encourage social distancing.
Students and staff who are unwell with acute respiratory symptoms or fever must not attend the university, and must self-isolate at home until their symptoms have resolved.
Universities and higher education centres should have contingencies in place to manage students who need to be quarantined or isolated if they are suspected of, or confirmed to be COVID-19 positive. It is important to note that group student accommodation presents a higher risk for transmission of COVID-19, similar to that experienced in boarding schools, and universities should have strategies in place to identify those who have respiratory symptoms or fever, and isolate these individuals as quickly as possible. If appropriate risk mitigation cannot be undertaken, universities and higher education centres should consider closing or reducing accommodation densities.
Recommendations to Residential Aged Care Facilities
While all respiratory viruses can cause outbreaks and significant morbidity and mortality, COVID-19 is acknowledged as a significant health risk particularly for the elderly and individuals with co-morbidities or low immunity.
While this recommendation is for RACFs, the principles are applicable to many settings including residential facilities for people with physical and mental disabilities, detention and correctional centres.
RACFs must ensure that they are prepared to manage outbreaks of COVID-19. Detailed guidance can be found at www.coronavirus-covid-19-guidelines-for-outbreaks-in-residential-care-f…. There is currently no vaccination to prevent COVID-19; avoidance of exposure is the single most important measure for preventing COVID-19 in RACFs. RACFs must have, and be vigilant in implementing measures to prevent introduction of COVID-19 into their facility.
Restrictions on entry into RACFs
The following visitors and staff (including visiting workers) should not be permitted to enter the facility:
- Those who have returned from overseas in the last 14 days.
- Those who have been in contact with a confirmed case of COVID-19 in the last 14 days.
- A contact is defined as anyone who has been in contact with a known case, including the 24 hours before the case became symptomatic.
- Those with fever or symptoms of acute respiratory infection (e.g. cough, sore throat, runny nose, shortness of breath) symptoms.
- Those who have not been vaccinated against influenza (after 1st May 2020).
Visitors
RACFs should implement the following measures for restricting visits and visitors to reduce the risk of transmission to residents, including:
- Limiting visits to a short duration;
- Limiting visits to a maximum of two visitors at one time per day. These may be immediate social supports (family members, close friends) or professional service or advocacy;
- Visits should be conducted in a resident’s room, outdoors, or in a specific area designated by the RACF, rather than communal areas where the risk of transmission to residents is greater;
- No large group visits or gatherings, including social activities or entertainment, should be permitted at this time;
- No school groups of any size should be allowed to visit RACFs.
Visitors should also be encouraged to practise social distancing practices where possible, including maintaining a distance of 1.5 metres.
Children aged 16 years or less must be permitted to visit only by exception, as they are generally unable to comply with hygiene measures. Exemptions can be assessed on a case-by-case basis, for example, where the resident is in palliative care.
Measures such as phone or video calls must be accessible to all residents to enable more regular communication with family members. Family and friends should be encouraged to maintain contact with residents by phone and other social communication apps, as appropriate.
Residents
Active screening for symptoms of COVID-19 in residents being admitted or re-admitted from other health facilities and community settings should be conducted. No new residents with COVID-19 compatible symptoms are permitted to enter the facility.
Residents admitted from other health facilities
Residents admitted from other health facilities should be assessed by appropriate medical staff prior to admission to the facility.
Appropriate infection prevention practices should be implemented for residents returning from treatment or care at other facilities.
External excursions
No external excursions for residents should currently be permitted.
Managing illness in visitors and staff
RACFs should advise all regular visitors and staff to be vigilant for illness and use hygiene measures including social distancing, and to monitor for symptoms of COVID-19, specifically fever and acute respiratory illness. They should be instructed to stay away when unwell, for their own and residents’ protection.
Given the high vulnerability of this particular group, RACFs should request that staff and visitors provide details on their current health status, particularly presentation of symptoms consistent with COVID-19. Screening for fever could also be considered upon entry.
These additional measures should be implemented in order to better protect residents and prompt individuals entering the RACF to consider their current state of health prior to entry. Both individuals and management need to take responsibility for the health of visitors and staff at facilities to protect our most vulnerable community members.
Symptomatic staff
Staff should be made aware of early signs and symptoms of COVID-19. Any staff with fever OR symptoms of acute respiratory infection (e.g. cough, sore throat, runny nose, shortness of breath) should be excluded from the workplace and tested for COVID-19. Staff must report their symptoms to the RACF.
Sick leave policies must enable employees to stay home, if they have symptoms of respiratory infection.
Hygiene measures
Signage and other forms of communication (i.e. information and fact sheets) must be used to convey key messages, including what actions the facility is taking to protect visitors, residents and staff, and explaining what they can do to protect themselves and their family members. This includes signs on appropriate hand washing techniques upon entry and throughout the facility.
RACFs must ensure that adequate hand washing facilities and alcohol based hand rub, as well as tissues and lined disposal receptacles are available for visitors to use; at the entrance of the facility and in each resident’s room. Staff should ensure visitors perform hand hygiene before entering and after leaving the resident’s room and the RACF.
The recommendations outlined may be altered according to the particular circumstance of the resident, including those who are in palliative care or residents in dementia units, which should be considered on a case-by-case basis. These situations will likely necessitate increased social contact with visitors.
Community sport
All community sport participants must play a role to help reduce the transmission of COVID‑19, including those organising, attending or supporting attendance at these activities.
Participants should not attend and participate in Community Sport if they:
- Have travelled internationally or been exposed to a person with COVID-19 in the preceding 14 days; or
- Are at a high risk including the elderly and those with pre‑existing medical conditions.
Attendance at community sport activities
Only essential participants should attend activities, i.e. players, coaches, match officials, staff and volunteers involved in operations and parents/guardians of participants;
All players, visitors should practise the following social distancing measures at Community Sporting activities:
- Players, visitors and officials should minimise physical contact as much as is practicable, for example no shaking hands, no walking out with player mascots, no pre- or post-match celebrations and no celebrating between players during the match.
- When spectating or attending a game or training session, ensure a distance of 1.5 metres is kept between yourself and others;
- Access to change rooms should be restricted solely to players, officials and essential staff;
- If spectating, try to maintain 1.5 metres between yourself and others.
- It is recommended that sporting teams, including school sporting teams, maintain local competitions only, with no inter-district, or inter-club travel. As with all gatherings, basic protective measures should be observed, such as regular hand hygiene practices before, during and after the match, do not share drink bottles, and avoid touching your face.
It is acknowledged that contact sports have a greater risk of transmission than other sports, and as such, should be considered on a case-by-case basis. However, other mitigation strategies for match socialisation and contact must be employed to reduce the risk to players, visitors, and officials more broadly.
Swimming pools
There is no evidence that the virus will survive in well managed and maintained pools chlorinated in accordance with Australian standards and guidelines. People should minimise time spent out of the pool and comply with the aforementioned social distancing and protective measures when in the change rooms and outside the pool. Shower with soap before attending the facility.
Recreational water facilities (water slides, surf parks) should also comply with social distancing and protective measures.
General hygiene measures at facilities
Facilities should:
- Ensure that spaces at each facility, surfaces and objects are regularly cleaned with disinfectant;
- Provide hand washing guidance (www.who.int/gpsc/clean_hands_protection/en/);
- Promote regular and thorough hand washing by staff and participants;
- Provide sanitising hand rub dispensers in prominent places around the event (particularly entry or high use areas such as a registration desk, change rooms, toilets or kiosk);
- Make sure dispensers are regularly refilled; and
- Promote exclusion of ill persons.
Recommendation on ANZAC Day ceremonies and events
ANZAC Day ceremonies and events should be cancelled due to the high proportion of older Australians who attend such events and the increased risk posed to such individuals. A small streamed/filmed ceremony involving officials at a state level may be acceptable. There should be no marches.
Recommendation on bulk purchase of supplies
The AHPPC advises against the bulk purchase of foods, medicines and other goods. We discourage the panic purchase of food and other supplies. While some advice has been provided to have a small addition of long shelf life products in the case of illness there are a range of mechanisms in place to support people in self-isolation, including food and other deliveries. AHPPC notes that the risk of individual Australians being asked to quarantine in coming weeks is low, and encourage individuals to plan with friends and family in the event of the need to isolate. We recognise the importance of supply lines to remote communities.