This statement has been archived.
Further short term social distancing measures
National Cabinet has asked AHPPC for advice on options for the progressive scale up of social distancing measures in response to the COVID-19 outbreak. There was a specific request to look at stronger measures in relation to non-essential gatherings initially, followed by further more intense options. The Cabinet has further asked for the triggers for introduction of stronger measures, either as a focal response or nationally.
The first thousand cases
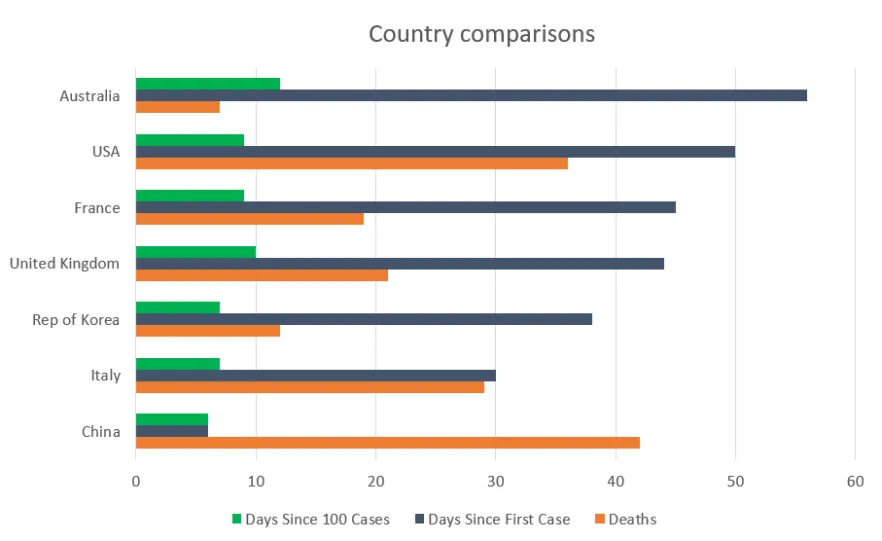
We now have 1,000 cases and we are clearly concerned at the rate of rise in cases and potential trajectory. Without diminishing the significance of the rise in case numbers, it is worth noting that the situation with our first 1,000 is somewhat different to that of other countries such as Italy and the USA when they were at 1,000. Please refer to the charts and table below.
More than half our cases are still imported from overseas or their direct contacts. We have one of the lowest COVID-19 test positivity rates in the world (0.9% compared to USA 13%, UK 5% and even ROK 3%). We have had only 7 deaths, all in people aged 75 or over and so far, less than 20 people have needed ICU treatment. This suggests that we do not have as large a proportion of undetected cases in the population, as was likely the case in the USA, Italy and other countries. Our early detection and control work was effective.
Current measures
Despite the above, the recent rapid influx in imported cases and associated chains of transmission, including cruise ships and super-spreader events, means we do need to do more now. It is too soon for the measures introduced only last week to have impacted on the epidemiology, but we are seeing evidence of non-compliance with these new measures, people not taking this seriously. We have also now had two ‘super spreader’ events in Sydney - one a wedding (35 infected) and one at a church service.
There is a strong argument to do more, at least in the short term, to enforce the new way of life in social distancing that we will have to endure and to adapt the Community mindset. This will also allow more time to consolidate health system preparations and evaluate measures already implemented in Australia, and to learn from interventions in other countries.
AHPPC supports national discontinuation of all non-essential gatherings
AHPPC recognises the importance of a nationally consistent approach to measures to reduce the spread of COVID-19. This would entail the temporary closure of registered and licensed clubs (excluding bottleshops attached to these venues), pubs, hotels (excluding accommodation), gyms, indoor sporting venues, cinemas, casinos, entertainment venues, restaurants and cafes (which will be restricted to take away and/or home delivery), places of worship, weddings, funerals (other than very small groups with the 4sqM per person rule to apply).
All of these restrictions apply to outdoor spaces associated with the above venues.
Isolated remote community hubs are not included in this closure.
Further restrictions may be considered as necessary.
These measures must be reviewed at one month. The duration of any measures must also take into account the changed trajectory of case numbers. If control is not strong at the end of one month, these measures may be continued for some months with some societal functioning. Effectiveness will depend on population-level compliance with social distancing and enhancements to case-finding, early isolation, contact tracing and quarantine.
These measures would also allow some of the health system preparedness concerns to be addressed, for the impact of the social distancing interventions implemented in mid-March to be assessed and future interventions to be planned.
AHPPC is also concerned about large informal outside gatherings and will come back to National Cabinet with more guidance. It is very important to encourage the community to adhere to social distancing outdoors, prior to the application of more stringent measures.
AHPPC does not support closure of schools at this time
AHPPC does not support the closure of schools given the lack of evidence of significant disease in children and the lack of reported major disease spreading in schools. Furthermore, the closure of schools poses a major risk to children's education, mental health and wellbeing, particularly those from low socioeconomic regions, where schools provide an important environment for nurturing and learning. The impact on the critical workforce and potential exposure of elderly relatives caring for children is also of significance. School closure would achieve some degree of additional social distancing but the evidence of its benefit at this stage is minimal. AHPPC views schools as an essential service and strongly supports keeping schools open.
There are significant opportunities to improve social distancing within schools, and we will continue to work to provide advice to the sector. AHPPC will continue to review developing evidence regarding the effect of the disease in children and the role of children in the transmission of the virus.
School closures are likely to be more effective when approaching the peak of the epidemic and enforced for a shorter period. If there is a strong desire to close schools at this later stage, it is essential that an option is provided for children of essential service providers, such as health care workers, to attend school or be otherwise cared for.
AHPPC notes one state has elected to bring forward their Easter school holidays.
AHPPC does not support full community lockdown at this time
Many countries have taken a total lockdown approach after having cases numbering in the thousands, and a growing number of deaths. Total lockdown is seen as the most dramatic way to limit spread. It entails citizens (other than essential service workers) staying a home, only going out for supplies or for medical attention. The aim is to reduce transmission to below R0=1 and stop the growth in cases in the short-term.
It is not clear what the strategy for paring back of restrictions should be. Proponents talk about relaxing these measures when control is achieved, by keeping the borders closed for over 12 months until a vaccine is developed. Other proponents have a narrative that a 4-6 week total lock down would enable greater focus on case detection and isolation, contact tracing and quarantine, and to consolidate preparedness of the health system.
The social disruption of this option is extreme and good compliance has generally required strong law enforcement/military presence. The public messaging of this would be challenging and need to ensure that it does not give false hope that any subsequent epidemic will either not occur or be materially modified as the long term effect of this intervention is unknown.
AHPPC recommends stronger enforcement of quarantine and isolation
The continued growth of cases in returned travellers (including the Ruby Princess) necessitates even stronger action on enforcing the quarantine of any returned traveller, with phone checks, mobile phone tracking and other measures. Similar attention needs to be given to case contacts in quarantine. Of most importance is the checking on the actual confirmed cases, if they are in isolation in their homes. It is not practical to keep them all in hospital but they must be checked daily with provision for formal supervised isolation for any non-compliance. Social support may also be required. This must include progressive expansion in the testing criteria, subject to availability of testing. Major supplementation of the public health workforce is in train and must continue.
Evaluation of efficacy of intervention
AHPPC will develop a suite of measures to assess the efficacy of all interventions. These measures will include:
- Evidence for efficacy of strengthened border measures/ travel advisories: reduction in the number of imported cases detected over time
- Evidence of efficacy of the reduction in non-essential gatherings and mixing group sizes: reduction in the average number of secondary infections per case, based in contact tracing
- Evidence for the combined efficacy of case finding and contact quarantine measures augmented by social distancing: reduction in the rate of growth of locally acquired infected cases
Urgent unintended matters will be addressed through ongoing reviews undertaken twice weekly at AHPPC and the National Cabinet.
Triggers for implementing further options
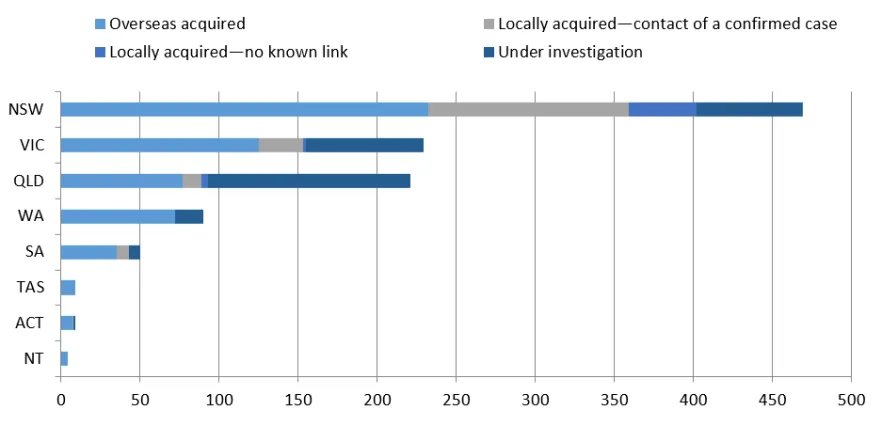
National cabinet asked if measures of case density in a given area would be a valuable guide to trigger further action. The spread of cases, however, while still mostly in large eastern seaboard cities is widespread across these cities. This is expected, given the preponderance at this stage of imported cases.
Previously AHPPC considered an important trigger in a given area to be when >50% of cases are locally transmitted, but recent international evidence suggests that action needs to be taken earlier than that point, given the lag in epidemiology. Nationally, Australia is close to 50% community transmission at this time but the major trigger is not focal. Rather it is the rapid growth in total cases and the case-load particularly in Sydney, Melbourne and Brisbane/Gold Coast. The call for action is now based on the principle of getting ahead of the curve the delay in the impact of new interventions.
A trigger for local lock down provisions in a part (or parts) of the country (as seen in Italy and elsewhere) would be a substantial growth in locally transmitted cases, which could be predicted to exceed the future capacity of the region’s health services. More modelling will be conducted to refine such predictive measures.
Recommendations
The growth trajectory of cases in Australia and the incomplete and slow implementation of social distancing measures, which is still a new concept for Australians, requires significantly stronger measures in social distancing in the short (initially for one month) term.
AHPPC recommends National Cabinet Consider immediately implementing the proposed stronger restrictions on indoor gatherings across Australia
AHPPC believes that school closures and full community lockdown should be held in reserve at this time with close daily review of the epidemiology.
Charts and table
First 1,000 cases – international comparison
As at 21 March there are 19 countries that have reported more than 1000 confirmed cases. The graph below compares 6 countries on the day they reported more than 1000 confirmed cases.
|
Country |
Cases |
Tests |
Percent COVID-19 positive |
Population |
Test by 100,000 population |
Date |
|
Australia |
1081 |
123,000 |
0.9% |
25,633,000 |
480 |
As of 21 March |
|
South Korea |
8565 |
282,555 |
3.0% |
51,470,000 |
549 |
As of 19 March |
|
UK |
3269 |
66,976 |
4.9% |
66,440,000 |
101 |
As of 20 March |
|
USA |
4484 |
54,205 |
8.3% |
327,200,000 |
17 |
As of 20 March |
|
Austria |
2013 |
18,545 |
10.9% |
8,822,000 |
210 |
As of 21 March |
|
France |
6153 |
36,747 |
16.7% |
66,990,000 |
55 |
As of 15 March |